Rethinking the Neurotological Approach
INTRODUCTION

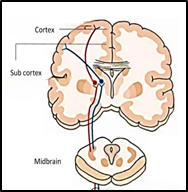
Both for diagnosis as well as for therapy, balance disorders are traditionally approached with a focus on vestibular labyrinths and brainstem reflexes. However, this approach is misdirected. The balance mechanism involves multiple organs and multiple systems. There is a hierarchical network for maintaining balance that involves cortical, subcortical, and brainstem centres. Not only that, the balance system also involves the ascending and descending columns in the spinal cord and the peripheral nerves of the lower limbs. Each part is equally important and a defect in any constituent of this neural network from the peripheral nerves in the lower most part of the body to the cerebral cortex in the highest level of the brain can lead to one or more of the vestibular symptoms of vertigo, dizziness, unsteadiness.
But the diagnostic tests and therapeutic focus is always limited to the vestibular labyrinths and the brainstem reflexes. For the maintenance of balance in activities of daily life, the visual and proprioceptive inputs are no less (rather, more) important than the vestibular labyrinths. When standing on the floor in a lighted room, more than 70% of the information required for maintaining balance comes from the proprioceptive system and not from the vestibular labyrinths. Despite this, both for diagnosis as well as for treatment, there is an unwarranted importance allotted to the vestibular labyrinths and the brainstem reflexes, and more often than not, clinicians are oblivious to the other more important constituents of the balance system. This tunnelled, if not perverted approach, camouflages the more important structures that actually control balance both in health and disease. This results in missing out the exact site of lesion, misdiagnosing the causative pathology and targeting the wrong regions of the body for therapy. The consequence of this wrongly directed diagnostic approach is a poor therapeutic outcome. Clinicians practising in neurotology need to shift clinical focus both as regards diagnosis and management from peripheral vestibular organs (the 3 semi-circular canals and the two otolith organs) and the brainstem reflexes (the vestibulo-ocular and the vestibulo-spinal reflexes) and look into other regions in the chain of organs and biological systems that control balance. Centres much higher up in the hierarchy of the central nervous system need to be targeted for a more effective diagnosis and a better therapeutic outcome. The control of balance, the clinical manifestations of a balance disorder, the degree of morbidity generated and concomitent non-vestibular manifestations in the domains of cognition, psyche and autonomic system are all operated by the cortex and subcortex which are the highest echelons of the central nervous syetem.

Clinicians practising in neurotology need to shift clinical focus both as regards diagnosis and management from peripheral vestibular organs (the 3 semi-circular canals and the two otolith organs) and the brainstem reflexes (the vestibulo-ocular and the vestibulo-spinal reflexes) and look into other regions in the chain of organs and biological systems that control balance. Centres much higher up in the hierarchy of the central nervous system need to be targeted for a more effective diagnosis and a better therapeutic outcome. The control of balance, the clinical manifestations of a balance disorder, the degree of morbidity generated and concomitent non-vestibular manifestations in the domains of cognition, psyche and autonomic system are all operated by the cortex and subcortex which are the highest echelons of the central nervous syetem.
THE MECHANISTIC BASIS
The processing and integration of the different sensory inputs viz the visual, proprioceptive and labyrinthine which are required for the maintenance of balance, take place in the cortex and sub cortex of the brain. Balance is not maintained only by the vestibular labyrinths, the labyrinths only detect movement of the head / body and inform the brain about the stability of the head in the torso in the linear and angular directions, but nothing much more. The brain needs to integrate this labyrinthine information with the information obtained from the eyes, the proprioceptors and even the interoceptors to maintain balance and to carry out the other functions of the vestibular system. After the multisensory integration, the cortex generates the requisite motor activity to maintain balance. The subject perceives this as visual and postural stability. It is this cortical processing that plays the decisive role in symptom generation, extent of morbidity, and quality of life issues in balance disorder patients. The highest echelons of the CNS where higher-order perceptive and cognitive functions are generated, is the place where the different sensory inputs for the maintenance of balance are integrated, processed, the most appropriate motor output as is warranted in that particular setting created and the feeling of stability or that of disequilibrium generated.
The vestibular labyrinth which are so hyped up in neurotology, are merely sensors (just like the eyes and the proprioceptors) that transduce mechanical energy generated by head / body movement into electrical signals for the cortical /subcortical structures to process the input. The brain stem reflexes i.e., the vestibulo-ocular reflex (VOR) and the vestibulo-spinal reflex (VSR) merely carry out the functions of gaze and postural stabilisation. But this too is dictated and controlled by the cerebral cortex. The executive function of very precisely contracting a selected group of muscles as required in a particular situation, factoring in past experiences stored in the vestibular memory is purely a cortical function. The vestibular labyrinths and the brainstem reflexes are not in any way responsible for the generation of the vestibular symptoms of vertigo/dizziness/ unsteadiness/ fear of falls and the different types of undesirable feelings / perceptions that a balance disorder patient experiences. Psychic, cognitive and autonomic systems all of which are controlled by the cortex come into play to generate the final perception / outcome of what the movement of the self / surroundings sensed by the different sensors generated in the patient. The vestibular labyrinths are just one of many sensors that sense the stability of the body but how the body is oriented vis a vis the surroundings is again a cortical function.
The Hierarchical Architecture of the Balance System
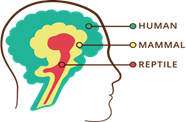
Vestibular function is organized across three interconnected levels:
- Lower brainstem (Ponto-medullary level): Reflexive control of gaze via the vestibulo-ocular reflex (VOR) and posture via the vestibulo-spinal reflex (VSR). These pontomedullary reflexes were made for reptiles to sense and respond appropriately to any danger
- Upper brainstem and cerebellar level: Sensorimotor control of voluntary movement and partial perception of motion.
- Cortical and subcortical level: Multisensory integration and generation of the precise motor output with economic utilisation of resources, spatial memory, bodily self-consciousness, motion perception, spatial navigation, autonomic corrections in accordance to the movement generated, and cognitive processing of balance.

In this hierarchical arrangement while vestibular labyrinths are essential as sensory organs, the perception of balance—and consequently the vestibular symptoms (vertigo/vestibulo-visual symptoms/dizziness /unsteadiness) and what the patient feels about his / her stability are generated by the highest level of the central nervous system i.e., the cortex and subcortex. There is a functional overlap between these three hierarchical levels but what the subject perceives about the self’s balance or orientation in relation to the surrounding space is limited to the cortex and subcortex.
Symptom Generation: Beyond the Labyrinth
The balance disordered patient presents to the doctor with a mix of vestibular and non-vestibular symptoms. The vestibular symptoms are head spinning or vertigo which may be internal (spinning sensation inside the head with the surroundings stable) or external (spinning / rotation of the surrounding visuals with the head stable), dizziness (i.e., a distorted feeling of the surrounding space, a feeling as if the self is not anchored to the physical surroundings) or unsteadiness or imbalance when the patient feels secure only when holding on to some physical support.


The non vestibular symptoms are difficulties in activities of daily life like bumping into others or into surrounding objects, autonomic/ cognitive /functional / psychic abnormalities and an agonising fear of fall or the dreadful feeling of an impending fall. However, none of these morbidities originate in the vestibular labyrinths or in the brainstem. These vestibular and non-vestibular symptoms are all feelings and perceptions or cognitive / psychic abnormalities, that can only be generated in the cortex and subcortex, mainly in the neocortex, hypothalamus & entorhinal cortex. These perceptions and feelings cannot be generated either in vestibular labyrinths or in the brainstem. What the patient feels about his/ her balance and perceives about the stability of the self are all generated in the cerebral cortex and subcortex. The origin of all vestibular symptoms be it internal or external vertigo, be it dizziness or unsteadiness is the cortex and the subcortex. While vestibular symptoms are often considered the primary targets for investigation and treatment, the vestibular symptoms are, in fact, perceptual phenomena—products of higher central processing rather than direct outcomes of peripheral vestibular dysfunction
Neurotological symptoms are generated predominantly when cortical structures are disturbed. The cortical functions may be jeopardised either due to any derangement in cortical functioning or it may be due to imperfect / erroneous inputs reaching the cortex from the vestibular labyrinths and other sources of afferent inputs like the visual or the proprioceptive input systems. Not more than 30% of above-mentioned vestibular symptoms arise from aberrant vestibular stimulation. The rest result from improper / inadequate inputs from the visual / proprioceptive systems but are primarily due to intrinsic defects in cortical or subcortical function. Even if there is a defective vestibular input, the highest levels of the CNS is smart enough to manage it by giving more weightage to the inputs from the other sensory organs and ignore or give less importance to the inputs coming from defective organs.
Central Processing and Morbidity

Defects in central processing can manifest as:
- Vestibular symptoms: Spatial disorientation (i.e., dizziness), internal vertigo, unsteadiness, vestibulo-visual abnormalities, and unreal sensations of self-motion or environmental motion.
- Non-vestibular symptoms: Cognitive impairments, psychic morbidity, emotional disturbances, autonomic symptoms, depersonalization, and derealisation.
Importantly, the non-vestibular symptoms often contribute more to the morbidity and the reduced quality of life of the balance disorder patient, than the primary vestibular symptoms themselves.
A critical clinical observation is that a patient may retain perfect balance perception despite vestibular deficits if central processing is intact. Conversely, patients may exhibit severe vestibular symptoms in the absence of measurable peripheral vestibular deficits—conditions such as Persistent Postural-Perceptual Dizziness (PPPD), Phobic Postural Vertigo, Visual Induced Dizziness (VID), and psychogenic vertigo.
Thus, a dichotomy exists between:
- Vestibular defects (sensory input level)
- Vestibular symptoms (perceptual level)
- Patient morbidity (functional and cognitive impact)
Cognitive Facets of Balance
Perfect equilibrioception involves complex cognitive faculties:
- Bodily self-consciousness
- Self-motion perception
- Spatial navigation and learning
- Spatial memory
- Object recognition memory
- Economic decision-making
- Numerical cognition
- Metric computations in 3D space

Each of these can be separately evaluated and quantified, offering valuable clinical insight beyond traditional vestibular testing.
Clinical Implications: What We Are Missing

Current clinical assessments often overemphasize the peripheral sensory organs (i.e., the vestibular labyrinths) while neglecting higher-order perceptive and integrative processes. This approach is not only incomplete but also potentially misleading.
To truly assess a balance disorder patient, clinicians must evaluate:
- Perception of motion thresholds (angular and linear)
- Spatial memory (e.g., Virtual Morris Water Maze, Corsi block test)
- Navigational ability
- Cognitive and psychological status (DHI, HADS, MoCA, MMS)
- Sensory inputs received from the proprioceptive system (by biothesiometry for vibration, qualitative temperature difference tests)
- Vascular systems of the lower limbs (e.g., Ankle-Brachial Index, Toe-Brachial Index)

A Paradigm Shift in Neurotology
We must evolve from “reptile-level” physicians, focused solely on reflexive brainstem functions, to “human-level” physicians, capable of comprehending and acting on the perceptive, cognitive and autonomic functions of balance. The latter take place in the cortical and subcortical levels far above the level of the brainstem level in the hierarchy of the central nervous system. Evaluating the higher CNS functions need to be imbibed into neurotological practice. The management of balance disorders demands a multidisciplinary, hierarchical approach that addresses not only the labyrinthine defects and the defects in the reflexive functions that occur in the brainstem level, but also derangements in central processing and cognitive / perceptive / psychic /autonomic ramifications. Not only the non-vestibular symptoms but also all the vestibular symptoms be it vertigo (internal / external), dizziness or unsteadiness are the result of erroneous processing in the highest levels of the CNS. Sometimes the deranged central processing may be triggered by defects in the vestibular labyrinths but more often they are the outcome of derangements of higher order cortical /subcortical processing
Conclusion
The perception of stability is a high-order CNS function, shaped by multisensory integration and cognitive processing. All vestibular symptoms as well as the non-vestibular morbidity perceived by a balance disordered subject is the outcome of defective central processing in the cortex / subcortex. A defective peripheral input does not always imply perceptual imbalance, and conversely, perceptual imbalance can arise from entirely normal sensory input i.e., even if the vestibular labyrinths are normal. Recognition of this central role of cortical and subcortical processing compels a rethinking of diagnostic strategies, shifting focus towards comprehensive, hierarchy-based evaluation in balance disorder management. This entails shifting clinical focus from the vestibular labyrinths and brainstem reflexes to higher order cortical and subcortical function as well as to other parts of the balance system like the visual / proprioceptive systems, the dorsal and lateral columns of the spinal cord through which the proprioceptive impulses reach the brain, the nerves and vascular structures of the lower limbs and more importantly to the cortex and subcortex .
Correspondence:
Dr. Anirban Biswas
E-mail: vertigodeafnesstinnitus@gmail.com
WhatsApp: +91 9830352580